
To write a credible and informative article, journalists endeavor to answer the “5 Ws”—Who, What, When, Where, and Why. While this approach to information-gathering is commonly associated with journalism, it is the framework of the Comparative Benchmarking System—a database of coded medical malpractice claims that provides insights into patient harm.
Claims in Candello are coded using a highly governed taxonomy that drives the capture and coding of event-related data from the medical and legal files associated with a medical malpractice claim. This process identifies key issues in clinical practice and system failures that lead to medical error and harm.
Over the decades, the CRICO taxonomy has evolved to incorporate current care practices, for example, human factor codes, electronic health records, and most recently, socioeconomic barriers and virtual care. The evolution of the taxonomy, along with the governance of its application, is what allows the data to be credible and reliable.
The purpose of CRICO's Clinical Coding Taxonomy is to support advanced analytic methods, with the ultimate goal of minimizing risk and enhancing patient safety. The Taxonomy serves as the analytic foundation of the Candello database, which allows the comparison of data broadly across multiple institutions.
THE “5 Ws” (and H) OF ADVERSE EVENTS
Coding medical malpractice claims enables organizations to analyze their data in order to gain insights into what went wrong and why. These insights enable health care leaders to make data-informed decisions. For example, it helps prioritize the most urgent needs or opportunities, and ensures the right people are involved in developing patient safety initiatives that will prevent similar events from happening in the future.
The multidimensional CRICO taxonomy supports the “story telling” of each medical event by answering these questions:
- What happened? This is the primary clinical focus of the case, or event. It provides a way to group common events, such as a surgical error, diagnostic error, falls, etc.
- Who was involved? This is a critical aspect of an adverse event as it will ensure that the right people are involved in understanding the issue and discussing ways to mitigate it.
- When did it happen? In the context of medical malpractice, this refers to when, during the process of care, the event took place. This could refer to pre-, intra-, or post-surgery, or perhaps pre-partum, labor, or post-partum.
- Where did it happen? Health care is delivered in a variety of locations from in-patient rooms, ORs and emergency department, to out-patient procedure rooms and the physician office. Location adds depth of understanding to the expected care team and processes, and the resources available in that setting. Events that may seem alike, such as falls, medication errors, or failure to rescue after a procedure, require different solutions depending where it happens.
- Why did it happen? Coded medical malpractice claims in Candello offer insights about the drivers of harm or contributing factors. This may include a human factor or a system breakdown. It might be clinical decisions made or the communication—or lack of communication—of those decisions.
- How was it resolved? Capturing the resolution of the medical malpractice claim can provided valuable data about claims management as well as help identify the costliest adverse events. In addition to capturing the verdict of claims that go to court, Candello also captures if a claim was dropped, denied, or settled. It including expenses associated with a claim, as well as the indemnity payment.
WHAT QUESTIONS CAN CLINICAL LEADERS ANSWER?
Being able to answer the “5 Ws” for a single event is integral to understanding that one specific event. This is often accomplished through a root cause analysis (RCA), which most risk managers are well-versed in performing. But often we need to understand trends from a larger data set in order to answer broader business questions, identify trends, or apply analytics and predictive modeling. Insights gained from the larger data set can inform priorities, resourcing, education, policy, etc.
The types of questions health care leaders look to Candello to answer include:
What happened?
- What types of clinical cases drive the volume of medical malpractice claims for my organization? How does that compare to organizations like mine?
- Which type of clinical case makes up the largest percent of lost dollars (expenses and/or indemnity)?
- What is the average cost of a specific type of case, for example, obstetric-related, or medication-related cases?
Who was involved?
- Which responsible service has the highest percent of high-severity outcomes? Is this the same for?
- Are cases that involve surgical spine issues more prevalent in orthopedics or neurosurgery?
- What percent of obstetrical-related cases involve a nurse practitioner?
Why did this happen, or why does it keep happening?
- How often does a communication-factor contribute to a kind of event, for example missed diagnosis?
- Are technical skill issues related to expected complication or to error? Is that ration, the same for attendings and residents?
- How often are cases impacted by failure to follow a policy?
The image below demonstrates how we look to Candello data to answer business and clinical questions. In this example, we queried Candello and applied predictive modeling to understand the impact of Patient Assessments on indemnity payments. Through analysis of the data, we start to understand the type of assessment failure (response to signs/symptoms, narrow diagnostic focus, etc.), the percent of cases that include that failure and the average indemnity paid. We also gain insights about the primary responsible services involved in cases that involve assessment failures, informing us who to involve in discussions as we develop initiatives to mitigate future risks.
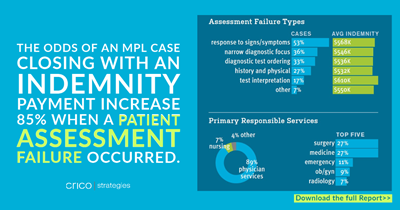
Image from the Power to Predict: Leveraging Medical Malpractice Data to Reduce Patient Harm and Financial Loss.(download full report)
You can read more examples of how Candello data has been leveraged to answer business, financial, and clinical questions:
- Medical Malpractice Data Findings for NPs and PAs
- Learning from Surgical Burn Adverse Events
- Medical Malpractice Data Propels Clinical Change
- Make Confident Business Decisions Informed by Data
- An Examination of Medical Malpractice Claims Involving Physician Trainees
If you are interested in learning how your organization can learn from its medical malpractice claims, reach out to us today.