
Millions of surgeries are performed in hospitals and ambulatory centers in the U.S. each year. While most of these procedures go smoothly, an unfortunate percentage result in patient injuries that include accidental tears, undetected infections, broken hips from post-surgery falls, and fatal complications. Along with pain and distress, some of these cases lead to medical professional liability (MPL) claims that cost the health care industry hundreds of millions of dollars annually.
To improve safety in surgical treatment, health care leaders must understand what went wrong and why, and then take action to fix the faulty or failed systems that have contributed to patient harm. We know that medical errors are rarely caused by a single missed step or event, but instead result from multiple missteps lining up.1 We also know that the vulnerabilities you identify in one service may be wreaking havoc elsewhere in your organization—compromising quality, undermining patient and staff satisfaction, hemorrhaging money, and hurting other patients.
In this analysis, we focus on key drivers of medical error in surgical treatment throughout the pre-operative, intra-operative, and post-operative periods, and we offer some interventions to help prevent them. Our insights are gleaned from 20-plus years of analyzing health care trends through a harm-and-loss lens. We have built a Candello database of more than 450,000 medical malpractice claims from captive and commercial insurers around the country, who collaborate in our Candello community. Our trove includes data from national hospitals, clinicians, as well as health care organizations within the Harvard medical community.
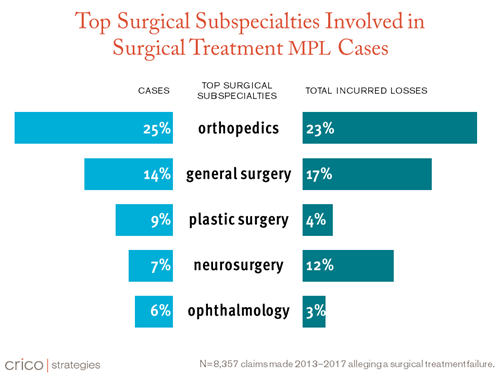
Our data tell us that surgical treatment remains the most common source of medical malpractice cases, and that these cases most frequently involve:
- clinical judgment or technical skill issues, with communication problems cited often as well;
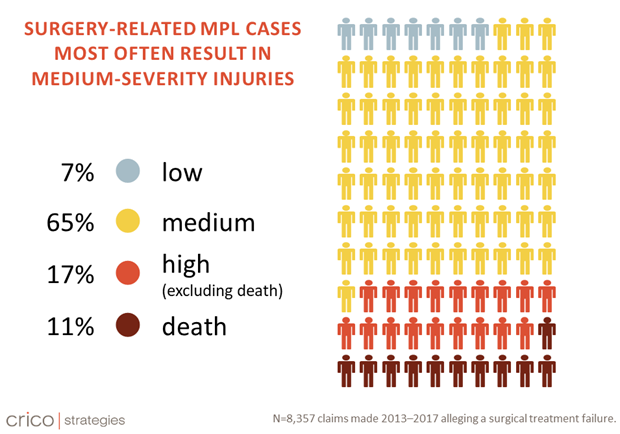
- medium-severity injuries; and
- five responsible services: orthopedics, general surgery, plastic surgery, neurosurgery, and ophthalmology.
As health care leaders, you are well-positioned to identify the services most responsible for surgical patients in your organization, encourage discussion about vulnerabilities, and develop solutions to address them.
TWO TYPES OF FAILURES
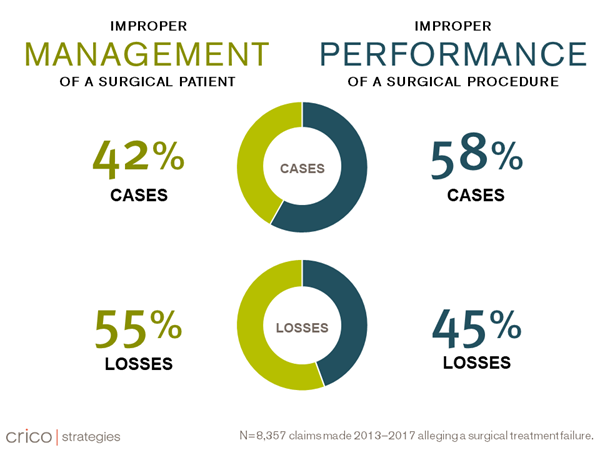
Our analysis of Candello data of surgical treatment injuries, outcomes, and contributing factors from 2013 to 2017 has revealed two general categories of MPL cases: surgery management-related and surgery performance-related. Several issues cut across both categories.
Surgical Management: These cases are most often associated with clinical judgment, such as overlooking an infection or failing to order a diagnostic test (both patient assessment issues). Communication gaps are also common contributing factors in surgical management. These may occur between providers and patients/families (e.g., not setting realistic expectations about potential complications) or among providers themselves (e.g., failing to read a patient’s medical record).
Surgical Performance: These cases typically stem from technical challenges, such as known possible complications that occur during or after a knee or hip replacement, poor technique in spinal fusion surgery, or retained foreign bodies. These performance-related cases may also involve clinical judgment (e.g., breakdowns in the selection or management of a procedure, or failure to respond to a patient’s signs and symptoms during surgery), and/or poor communication—for example, inadequate informed consent.
It’s interesting to note that although cases involving improper performance make up nearly 60% of the surgical cases in our MPL database, they comprise a smaller share of financial losses (45%) than those involving improper surgical management (55%).
MULTIPLE FACTORS
As with other industries, mistakes or near-misses in health care usually involve more than one coexisting system or process; in fact, our 2018 annual report, which analyzed a decade of MPL data from 2007 to 2016, revealed an average 3.3 contributing factors per case.
No one weakness or failure brings down the house; it’s usually a mix of contributing factors. This underscores the need for leadership to look well beyond the vulnerabilities that surface in one unit or department.
Similarly, surgical treatment failures typically reflect a complex interplay of breakdowns in clinical judgment, technical/procedural issues, and communication. Take, for example, an unintended laceration during surgery that results in a slow bleed, or a bowel perforation that leads to a slowly growing infection (technical issues). If your post-op assessment or differential diagnosis is too narrow (clinical judgment issues), and/or if any team member doesn’t communicate symptoms quickly, efficiently, or at all because they did not recognize them (communication issues), the patient’s status can quickly worsen.
INJURIES
Our data also tell us that surgery-related cases most often result in medium-severity injuries—that is, harm that is major but temporary, or minor but permanent. These might include punctures/perforations, injury to an adjacent organ, or nerve damage during surgery, as well as infections (surgical site or systemic), blood clots, or bleeding after surgery.
Compared to other breakdowns in quality care, such as diagnostic failures, surgical-related injuries are more readily identifiable during the procedure or in post-op. This may enable a faster response and minimize long-term health consequences to the patient.
The types of injuries that can occur in these cases highlights the importance of clear and complete communication with patients and families throughout the entire perioperative period, from the pre-operative education and consent process, to the immediate and long-term recovery process.
In the event that an unexpected outcome or complication occurs, leaders should support and empower providers to see through the proper disclosure process. It is critically important to educate providers and clinical teams about the potential impacts of surgical errors and to encourage them to report events and near-misses to leadership to facilitate learning and improvement.
CLAIMS AND PAYMENTS
About one-third of all surgical cases close with payment, with an average indemnity of approximately $350,000. While just over half of MPL cases occur in the inpatient setting, it’s no surprise that ambulatory-based cases are becoming more prevalent as the industry shifts toward more outpatient care. Leaders who understand the contributing factors that precipitate these complaints are better positioned to identify risk management strategies tailored to each setting.
IDEAS FOR MITIGATION
Reducing the risk of patient harm in surgery requires three “C”s: collaboration, consistency, and communication. Here are some intervention ideas, gleaned from our two decades of experience coding and comparatively analyzing medical malpractice claims, and providing improvement recommendations to our Candello clients:
Collaboration
- Engage all clinicians and other staff across your surgical service by providing data and case studies highlighting key risk areas.
- Facilitate cross-disciplinary discussions about potential improvement strategies.
- Support and empower clinicians at all levels to report events and near misses to leadership to facilitate learning and improvement.
Consistency
- Assess your processes for receiving, reviewing, and documenting critical pre-operative information, including history and physical exams, consults, and test results.
- Standardize your pre-operative assessment procedures for patients with specific histories and comorbidities. This includes coordinating with consultants to ensure readiness/surgical clearance for each identified comorbidity.
- Ensure consistent use (and documentation) of informed consent protocols and patient education tools like Emmi to promote accurate expectation setting.
- Implement, sustain, and reinforce sepsis response pathways across surgical disciplines.
Communication
- Provide clear and complete communication with patients and families throughout the surgical process, from consent to long-term recovery.
- Consider developing communication triggers, such as clinical criteria that require nurses, residents, and consultants to contact the attending physician if a patient’s status changes.
- Ensure that staff use tools to support effective patient handoffs, such as I-PASS, a pneumonic (memory aid) to standardize the handoff process.
- Assess whether cultural factors, such unprofessional behavior, or other factors affecting psychological safety, are impeding successful communication among clinical team members.
We are dedicated to helping our Candello community of peers improve patient safety practices and reduce litigation risk through a data-driven, learn-from-our-collective-experiences approach. Uncovering the drivers of patient harm in surgery and beyond is foundational to our work, and we look forward to sharing our insights with you in future blog posts.
References
Patient Safety and Quality Healthcare(PSQH). "I-PASS and SBAR Handoff Tools Have Proven Benefits." April 13, 2016. Accessed November 2, 2020. htpps://www.psqh.com/news/i-pass-and-sbar-handoff-tools-have-proven-benefits/
This analysis originally published November 5, 2020.