
The relationship between malpractice risk and important factors, such as physician specialty[1],[2] and prior malpractice history,[3] have been explored in the medical literature. However, little was known about how clinical volume, a fundamental aspect of clinical practice, factors into physicians’ risk of facing malpractice claims.
RELATIONSHIP BETWEEN CLINICAL VOLUME AND MEDICAL MALPRACTICE EXPOSURE
We recently examined how clinical volume affects medical malpractice risk. We explored this relationship by joining CRICO’s malpractice claims data with a database containing information on physician billing.[4] We used the physician billing database to generate information on how busy each physician was by measuring how many patient encounters each physician had, and how much they billed.
Our analysis of the annual risk of a malpractice claim as a function of how much the physician billed demonstrated that the more each physician billed, the greater their annual malpractice risk. This result was not unexpected since, for each patient encounter, there is the possibility of an adverse event that could lead to a malpractice claim. Thus, the more clinical activity a physician has over the course of a year, the greater the malpractice risk during that year.
The more interesting question we tried to answer was: what is the per encounter risk of a malpractice claim as a function of clinical volume? This is the question that is most relevant to patients because, as a patient, one is interested in how the malpractice risk associated with a given encounter varies depending on how busy the physician is.
Prior research has demonstrated that, for both individual physicians and at the hospital level, performing a higher number of procedures is associated with a lower per-procedure risk of a poor outcome. In essence, when it comes to the volume of procedures in medicine, more practice makes you more proficient.
Similarly, what we found is that less busy physicians had a higher per encounter risk of a malpractice claim and, the lower the volume, the higher the per encounter malpractice risk. The per encounter malpractice risk as a function of clinical volume leveled off once the physicians were above the bottom quarter of least busy physicians.
Intriguingly, when we graphed the relationship between per encounter malpractice risk and clinical volume (shown on the left) we realized that the graph had a familiar appearance.
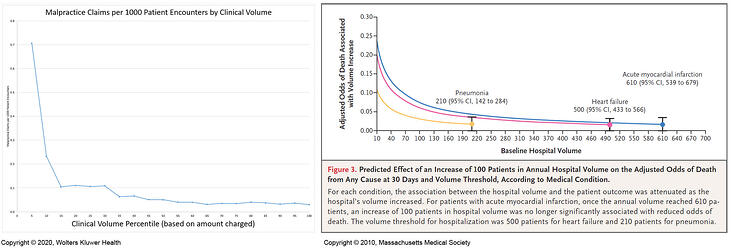
This appearance—in which, below a certain clinical volume threshold, the risk of the adverse outcome increases as clinical volume decreases but is stable above that threshold—has been seen in multiple studies of the relationship between the rate of adverse outcomes and clinical volume.[5],[6] Among the studies in which this relationship has been demonstrated is a prominent paper published in the New England Journal of Medicine, from which the graph on the right is reprinted, on how the 30-day risk of death for common medical conditions varies with the clinical volume of the hospital.[7]
MPL DATA FOR PATIENT SAFETY RISK IDENTIFICATION AND PROGRAM EVALUATION
The utility of medical professional liability (MPL) data in pinpointing patient safety risks and suggesting mitigation strategies is well established. Examples include predefined triggers for communication between resident and attending surgeons[8] and the I-PASS handoff system.[9] Malpractice data pointing to the importance of communication failures helped catalyze both of these patient safety innovations.[10],[11]
However, the remarkable similarity between how malpractice risk per encounter varies as a function of clinical volume and how the rates of commonly measured adverse events (such as surgical complications and death) vary at different levels of clinical volume highlights another use for malpractice data—serving as a proxy for adverse clinical outcomes more generally. In other words, malpractice data can be used not only to identify where our patient safety efforts should be targeted, but these data can also help us evaluate the effectiveness of patient safety programs that have been implemented.
This is a novel use of malpractice data that has so far been applied principally to patient safety programs within obstetrics and gynecology,[12],[13] in part because of the relatively high malpractice rates within this specialty. The use of malpractice claims data in program evaluation is something we should expect to see more off in the future.
Candello Members can watch a recording of Dr. Schaffer presenting the original research from the paper, The effect of clinical volume on annual and per-patient encounter medical malpractice risk, in the online Community. (Note: The online Community is for Candello Members only.)
References
[1]Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. New England Journal of Medicine. 2011;365(7):629-636.
[2] Schaffer AC, Jena AB, Seabury SA, Singh H, Chalasani V, Kachalia A. Rates and characteristics of paid malpractice claims among U.S. physicians by specialty, 1992-2014. JAMA Internal Medicine. 2017;177(5):710-718.
[3] Studdert DM, Bismark MM, Mello MM, Singh H, Spittal MJ. Prevalence and characteristics of physicians prone to malpractice claims. New England Journal of Medicine. 2016;374(4):354-362.
[4] Schaffer AC, Babayan A, Yu-Moe CW, Sato L, Einbinder JS. The effect of clinical volume on annual and per-patient encounter medical malpractice claims risk. Journal of Patient Safety. Epub ahead of print, March 23, 2020.
[5] Holt PJ, Poloniecki JD, Khalid U, Hinchliffe RJ, Loftus IM, Thompson MM. Effect of endovascular aneurysm repair on the volume-outcome relationship in aneurysm repair. Circulation: Cardiovascular Quality and Outcomes. 2009;2(6):624-632.
[6] Adam MA, Thomas S, Youngwirth L, et al. Is there a minimum number of thyroidectomies a surgeon should perform to optimize patient outcomes? Annals of Surgery. 2017;265(2):402-407.
[7] Ross JS, Normand S-LT, Wang Y, et al. Hospital volume and 30-day mortality for three common medical conditions. New England Journal of Medicine. 2010;362(12):1110-1118.
[8] ElBardissi AW, Regenbogen SE, Greenberg CC, et al. Communication practices on 4 Harvard surgical services: A surgical safety collaborative. Annals of Surgery. 2009;250(6):861-865.
[9] Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. New England Journal of Medicine. 2014;371(19):1803-1812.
[10] Candello. Malpractice Risks in Communication Failures. Boston, MA, 2015.
[11] Ross J. Effective communication improves patient safety. Journal of Perianesthesia Nursing. 2018;33(2):223-225
[12] Austin N, Goldhaber-Fiebert S, Daniels K, et al. Building comprehensive strategies for obstetric safety: Simulation drills and communication. Anesthesia and Analgesia. 2016;123(5):1181-1190.
[13] Pettker CM, Thung SF, Lipkind HS, et al. A comprehensive obstetric patient safety program reduces liability claims and payments. American Journal of Obstetrics and Gynecology. 2014;211(4):319-325.
Photo Credit:
Schaffer AC, Babayan A, Yu-Moe CW, Sato L, Einbinder JS. The effect of clinical volume on annual and per-patient encounter medical malpractice claims risk. Journal of Patient Safety. Epub ahead of print, March 23, 2020.
New England Journal of Medicine, Ross JS, Normand S-LT, Wang Y, et al., Hospital volume and 30-day mortality for three common medical conditions, 2010;362(12):1110-1118. Copyright ©2010 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
Written By
