
Embolisms and thrombosis may represent a small percentage (2.58%) of all medical malpractice cases in our Comparative Benchmarking System (Candello) but they can be catastrophic for the patient. The following analysis was conducted using our Clinical Event Search Engine, which queries closed medical malpractice claims in Candello.

EMBOLISM/THROMBOSIS MPL CASES ACROSS CARE SETTINGS
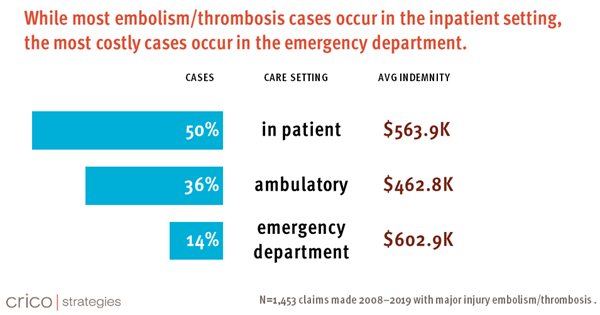
In an analysis of national medical malpractice claims in the Candello over a ten-year period (2008-2019), the majority of medical malpractice cases with an embolism/thrombosis as the major injury occurred in the inpatient setting (50%), followed by ambulatory setting (36%), and finally the emergency department (14%).
This is in line with research that has found that more than half of venous thrombosis embolism (VTE) cases, which encompass deep vein thrombosis (DVT) and pulmonary embolism (PE) are associated with a recent hospitalization or surgery.1
THE COST OF EMBOLISM/THROMBOSIS MPL CASES
Venous thrombosis embolisms can be catastrophic for the patient as we can see in the level of severity of these cases in Candello. Nearly half (47.4%) of the 1,453 cases in Candello with a major injury of embolism/thrombosis involve a patient death, while 26.6% are high severity and 25.5% are low severity.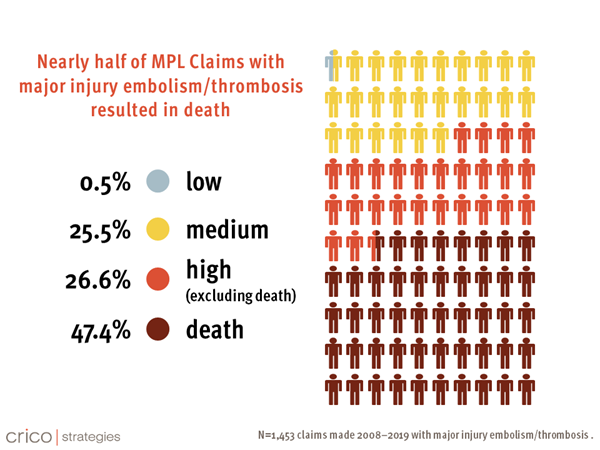
Across care settings, 39.1%of the embolism/thrombosis-related medical malpractice cases close with an indemnity payment, with the average payment of $529k. While the rate of the cases that closed with a payment is on par with all cases, the average indemnity payment is 41% more than the average indemnity payment of all cases in Candello.
Indemnity payments for embolism/thrombosis cases vary across the three care settings of inpatient, ambulatory and emergency department. Even though fewer embolism/thrombosis malpractice cases occur in the emergency department, the average indemnity of these cases is highest in this setting.
CONTRIBUTING FACTORS BY CARE SETTING
Evaluating the failures driving these cases assists patient safety professionals and providers in developing action plans to mitigate the risk of VTEs. Among the top five contributing factors across the inpatient, ambulatory, and emergency department care settings, patient assessment issues appear in all three settings. More specifically, the contributing factors identify failure to appreciate and reconcile relevant sign/symptoms/test results and failure to order a diagnostic test in varying degrees across the care settings.
|
Inpatient (n=727) |
Ambulatory (n=521) |
Emergency Dept. (n=205) |
|
|
|
Understanding the drivers of risk among each care setting might provide actionable information for the health care leaders tasked with working on mitigating the risk of VTEs across these settings.
INTERVENTIONS
Four areas that are frequently considered to minimize VTEs include patient assessment, prophylaxis, education, and process measures. A deeper understanding of the drivers of risk and harm associated with VTEs positions health care leaders and clinicians to make a data-informed decision about risk mitigation strategies.
There are many resources that can support the next step of your risk mitigation strategy. Below are some references from the The Centers for Disease Control (CDC) and the Agency for Healthcare Research and Quality (AHRQ) as well as closed medical malpractice case studies from CRICO.
References
- Centers for Disease Control and Prevention. “Learn About Healthcare-Associated Venous Thromboembolism.” Page last reviewed February 7, 2020.
- Agency for Healthcare Research and Quality (AHRQ). "Preventing Hospital-Associated Venous Thromboembolism.” Page last reviewed August 2016.
- CRICO. “Narrow Focus Fogs Opportunity for Timely PE Diagnosis.” April 30, 2020.
- CRICO. “Woman Dies from Post-op Stroke when Anticoagulant Not Restarted”. December 17, 2020
- CRICO. “'What Else Might This Be?' Might Have Saved PE Patient.” July 20, 2020.