
A recent medical malpractice case was in the news alleging a patient was burned in the operating room. It named two surgeons, a nurse and anesthesiologist and alleged that fire prevention protocol was not followed. I was curious to know more about his type of alleged malpractice, such as how frequently does this occur and what can be learned from this type of event in order to prevent future occurrences?
I ran a query of our Comparative Benchmarking System (Candello)—a database of deeply coded national medical professional liability (MPL) cases—using a new tool we are beta testing with our clients. The tool gives quick access to search for similar cases to an event that an organization may have experienced, such as a patient burn.
Looking at closed claims over a 10-year period (2008-2019), the data set found 275 malpractice cases that had the top major injury of a burn during a surgical event. That represents approximately half a percent (0.49%) of all surgical-related cases in this 10-year period. Not a significant amount.
If you have one event that happens, your intervention will likely address the root causes of that one event. But looking at a larger data set of similar events and the contributing factors driving these events, you might be able to address larger systemic issues. So, what can we learn from these 275 cases?
WHAT CAN WE LEARN FROM CASES LIKE THESE?
As a former chief nursing officer, I oversaw root cause analyses (RCAs). What was frustrating for all of us involved, was to think we addressed the issue(s) only to have a similar event happen a year or two later. Why didn’t our intervention work?
Learning from an isolated event is an integral part of risk management, however understanding the drivers of this kind of event on a larger scale can help put the event into perspective.
Looking at this data query, the top contributing factors associated with 275 surgical treatment closed malpractice cases that involved a patient burn (2008-2019) were:
- Improper use of equipment (includes user error) (32.4%)
- Selection/management of therapy (22.5%)
- Technical issues (21.5%)
- Patient monitoring – physiological status (other than med response) (16.0%)
This list of contributing factors helps me understand that technical issues and proper training of equipment is highly relevant in preventing patient burns during surgical procedures.
ANOTHER SLICE OF THE DATA
Using this tool, I can look at this from another angle: How often does this injury result in surgical cases compared to all burn injuries?
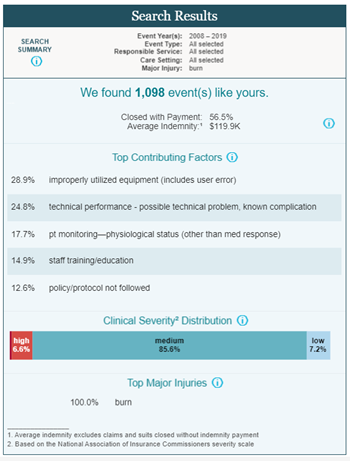
We know that there are 275 surgical cases that resulted in burns in this data set. When look at all burn injuries (using the same time frame), there are 1,098 cases. This provides more perspective: surgical-related burns (275 cases) represent 25% of all burn injuries (1,098 cases) in this data set.
The top contributing factors are similar however, staff training/education (14.9%) and policy/protocol not followed (12.6%) are present as contributing factors.
Another way to look at this type of injury is to see how frequently the named responsible services are involved in burn injuries. In the case mentioned in the news, the responsible services named in the suit included nursing, surgery and anesthesiology.
Using our Candello tool, I looked at these responsible services and you can see blow that improper use of equipment , issues with policy/protocols, and patient monitoring are the most prevalent factors driving these cases across the responsible services.
| Nursing | Anesthesiology | Surgery-General | Surgery-Sub-specialty |
|
|
|
|
LEVERAGING THE DATA FOR INTERVENTIONS
As you can see, expanding my research beyond the one case has shown the event through a broader lens. This is integral to being able to better understand systemic or process issues.
In the legal case mentioned earlier, the claim alleges a contributing factor is that a policy/protocol was not followed. Based on this one case, the action plan would focus on the policy/procedure that was not followed (e.g., why was it not followed, is the policy reasonable, do staff know about the policy?).
However, the information gained from a larger data set illustrates other driving factors in similar cases. These other contributing factors (improper use of equipment; patient monitoring) should be considered when developing an action plan even if they did not influence the outcome of this specific case. This will ensure that you are reducing the risk of a similar event happening.
Based on these data findings, I might look for interventions that could address these issues on a macro level across these responsible services thereby possibly reducing the risk of more than just burn injuries in the surgical setting.