
I remember back to when I was a bedside nurse, a time when patients, families and visitors treated health care workers with the utmost respect. They were grateful for the compassionate care provided at some of the worst times in their lives. Unfortunately, the same is not true today. Hard working people who chose health care as a profession and made a commitment to help others are being physically assaulted, verbally abused, or threatened by patients, family members and visitors every day. Not surprisingly, WPV has been a top patient safety concern for many years from trusted sources such as ECRI, Becker’s, OSHA, and AHA.
According to the Occupational Safety and Health Administration, “nonfatal workplace violence [WPV] is more widespread in the Healthcare and Social Assistance Standard than in any other industry”. Additionally, according to the Bureau of Labor Statistics and the Association of American Medical Colleges, health care workers have faced a significant increase (63% from 2011–2018) in the incidence of violent and aggressive acts in the workplace. More alarming, a January 2023 report published by the Massachusetts Hospital Association (MHA) in support of a statewide Call to Action for Patient and Visitor Codes of Conduct, indicates the state has seen a steep rise in violence at Massachusetts Healthcare Facilities with an incident occurring on average every 38 minutes in 2022, as compared to 2020 and 2021 when the estimated rates were 57 and 49 minutes respectively. Sadly, this is probably grossly underestimated as OSHA and The Joint Commission (TJC) indicate that most healthcare worker assaults go unreported. The staff have simply learned to accept this as part of their job.
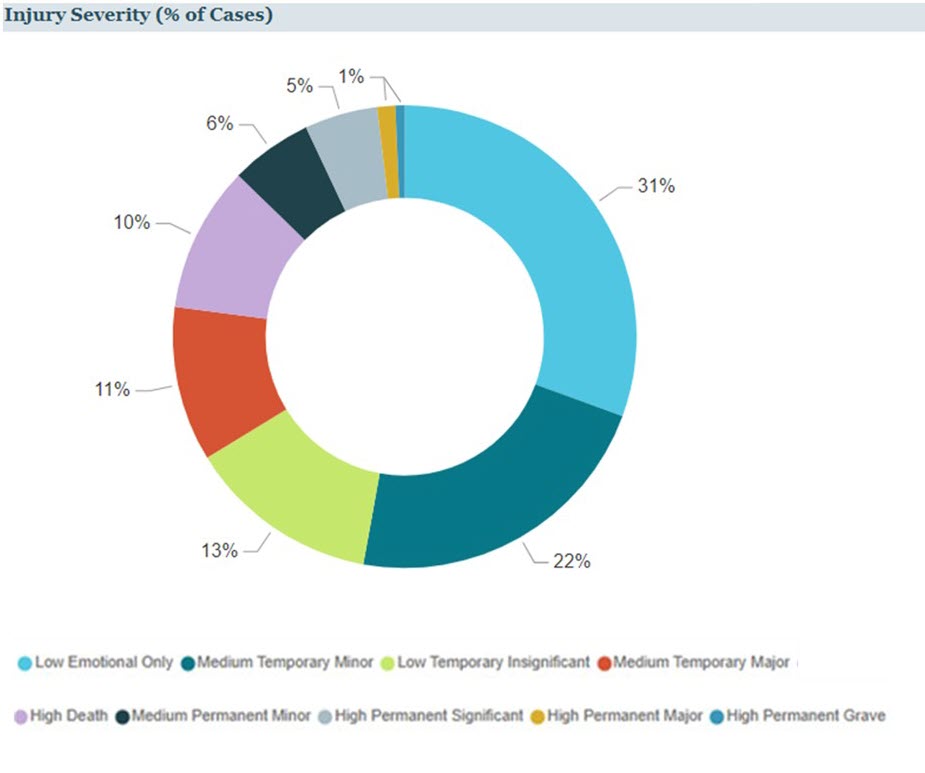
WPV can occur in any clinical area, however most events occur on inpatient behavioral health units or the Emergency Department (ED). A review of Security and Safety events in the Candello database from 2018 – 2023 revealed 157 cases with a major allegation subcategory of failure to protect from assault or security/assault, with total incurred losses of $30,000,000.
Candello Data Provides Valuable Insights on Security and Safety Events
(Samples from the Candello Explore tool)

|
|
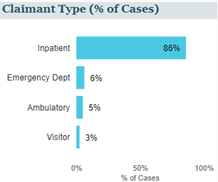
Out of 157 cases, 135 (86%) occurred in the inpatient area and 10 (6%) occurred in the ED. |
|
Additionally 17% (27) resulted in high severity injuries including death (10%). |
 |
Data complied by Michelle Bondurant, RN, CP, Coding Manager, Candello
Even if a healthcare worker is not the direct target of the physical assault or verbal abuse, they are being exposed daily to violence between and among patients. Hospitals and clinics are obligated under federal and state regulations to provide care to ALL patients, even those who are unruly and disruptive, making it nearly impossible to terminate or transfer care for even the most violent and aggressive patients, a fact that is not lost on today’s healthcare consumers. Many states have enacted laws making assault and/or battery against a healthcare worker a felony punishable by imprisonment or fine. However, when staff make the decision to call in law enforcement to assist with the situation and/or to file charges against the perpetrator, things can get tricky. While I thoroughly support our healthcare workers in exercising their rights under the law, law enforcement personnel are not well versed in the regulations by which hospitals must abide. Law enforcement officers, in doing their job, may put hospitals or facilities with dedicated emergency rooms at risk of possible violation of federal EMTALA regulations by removing a patient seeking emergency treatment or labor and delivery services from the premises prior to receiving a medical screening examination. This could result in substantial monetary penalties for the facility or costly medical malpractice claims for failure to treat.
Sadly, most healthcare workers often just stand by and take the verbal abuse, physical assault, or threatening behavior out of respect for the patient or possibly in fear of losing their job, but some are beginning to defend themselves. While I certainly do not support healthcare workers physically or verbally assaulting patients, you have only to watch one video of a patient or visitor viciously hitting, kicking, punching, spitting at, or strangling (yes, strangling!) a nurse, nursing assistant, licensed independent provider, security officer or other healthcare worker to understand why they may feel the instinctual need to defend themselves. Equally as disturbing is that some patients/visitors have taken to videotaping healthcare workers without their consent or knowledge during these interactions and then posting on social media, but not always depicting the full story, further fueling the violence.
The impact of WPV on health care workers not only impacts their physical safety but also takes a toll on mental well-being. Many staff already under the tremendous strain of the pandemic and resulting staffing shortages, are electing to remove themselves from the workforce due to the increasing violence.
Due to hospital accreditation standards such as the Joint Commission (TJC) or Det Norske Veritas (DNV), and recommendations by regulatory organizations such as OSHA, many hospitals have taken a comprehensive approach to developing health care violence prevention programs aimed at ensuring staff and patient safety. Some common WPV prevention best practices include: providing de-escalation training for all staff; posting highly visible signage warning patients and visitors that violence will not be tolerated, and that law enforcement may be called; providing personal panic alarms; implementing staff well-being rounds; utilization of a systemwide or statewide alert systems to identify repeat offenders; creation of behavioral health emergency response teams; and conducting post incident debriefing with peer support. While these interventions are critically important and send a strong message of support to health care workers, they often do little to prevent the violence in the moment making staff feel ever vulnerable even in facilities with a strong WPV prevention program.
Abuse and violence should not ever be considered “one of the hazards of the job”. We need to stand up and support those who have devoted their lives and careers to helping others in their time of need. The topic of workplace violence has been a focal discussion point in the Candello Patient Safety Study Group, one of the many opportunities for community members to connect with national peers and share insights and ideas, proving collaboration to be a vital tool for improving patient safety. Learn more about Candello’s national community and convening opportunities.
References
- Injuries, Illnesses, and Fatalities. www.bls.gov. https://www.bls.gov/iif/home.htm
- Boyle P. Threats against health care workers are rising. Here’s how hospitals are protecting their staffs. Association of American Medical Colleges. Published August 18, 2022.
- Workplace Violence SBREFA | Occupational Safety and Health Administration. www.osha.gov.
- Massachusetts Hospital Association. MHA Members Issue a United Call to Action on Violence in Healthcare Facilities. 2023, January 30.
Written By
